
Keith Chan is a New York State licensed physical therapist at ITNYCPT in New York City. He uses this format in all patient visits. This helps keep medical records accurate and supports continuity of care.
Key Takeaways
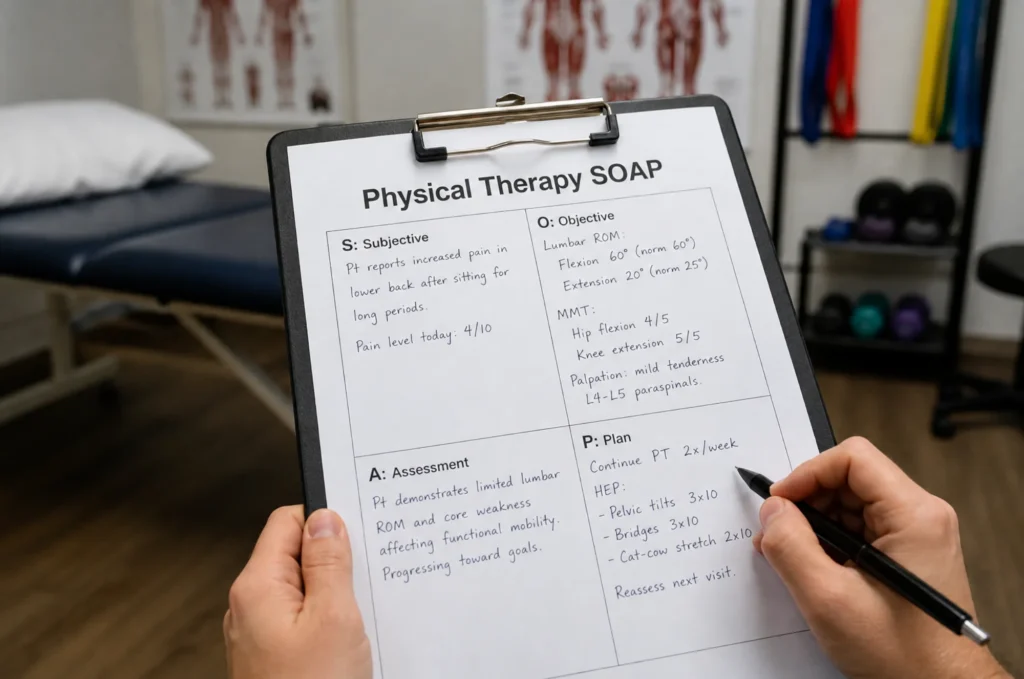
- A physical therapy SOAP note is a legal and clinical document that records what happened during a session across four sections: Subjective, Objective, Assessment, and Plan, each with a distinct purpose.
- The objective section requires specific, measurable data, including ROM degrees with normal reference values, manual muscle testing grades, and standardized outcome measures such as the Oswestry Disability Index, to demonstrate patient progress over time.
- The assessment section is the most commonly underdocumented part of a SOAP note; it must interpret clinical findings and connect them to functional goals, not simply restate what happened during the session.
- Daily SOAP notes, initial evaluation notes, and progress notes are three separate documents that serve different purposes, and conflating them is one of the most common billing errors in outpatient PT practice.
- Every session note must justify medical necessity by showing that the patient’s condition required the skill level of a licensed physical therapist, not just the completion of a home exercise program.
What Is a SOAP Note in Physical Therapy?
A physical therapy SOAP note is a written record of a single patient encounter. It documents what the patient reported, what the therapist measured and observed, the therapist’s clinical interpretation, and the plan for the next phase of care. SOAP stands for Subjective, Objective, Assessment, and Plan, and each section has a distinct purpose.
Physical therapy notes support communication among providers, help physical therapists track progress throughout the full plan of care, and demonstrate that treatment decisions were clinically justified — which matters especially when patients are asking how long physical therapy takes and what progress looks like at each stage.
The American Physical Therapy Association identifies two leading causes of claim denials: failure to demonstrate medical necessity and failure to document skilled care. Understanding billing standards, such as the 8-minute rule in physical therapy, is part of writing notes that hold up to payer review.
Every session note needs to answer one question: why did this patient need a licensed physical therapist today?
What Each Section of a PT SOAP Note Contains
The four sections of a SOAP note each capture a different type of clinical information. Understanding what belongs in each section of a SOAP note is the foundation of accurate, defensible documentation.
Subjective: What the Patient Reports
The subjective section records what the patient tells the therapist. It includes the chief functional limitations, current pain level, and response to past treatment.
It also records relevant medical history. This gives the therapist context to understand the patient’s condition. It shows how past health events may affect the current care plan.
Objective: What You Measure and Observe
The objective section records measurable, observable data. Every entry should be quantifiable and reproducible. This is where range-of-motion measurements, strength grades, special test results, and intervention details are documented.
Entries should be specific. “Knee flexion ROM: 95 degrees (normal: 135 degrees)” is useful. “Limited range of motion” is not.
For strength, use the standard 0-5 manual muscle testing scale. For functional outcomes, include standardized tools such as the Oswestry Disability Index for back pain, the Lower Extremity Functional Scale, or the Visual Analog Scale for pain, and record both baseline and reassessment scores to demonstrate progress over time.
Assessment: Your Clinical Reasoning
To properly assess the patient, the therapist interprets the subjective and objective findings together rather than restating them.
A strong assessment answers three questions: what is the patient’s current clinical status, how are they progressing toward their functional goals, and what justifies continued skilled physical therapy?
It should address the patient’s condition directly and connect measurable findings to real-world function, including documenting any reported pain after physical therapy sessions, which is clinically relevant to the assessment and plan.
Plan: Next Steps and Goals
The plan section describes what happens next, including session frequency, home exercise instructions, referrals, and any adjustments to the patient’s treatment approach. Every item should point to an actionable step.
How to Write Each Section
Writing SOAP notes well requires a different focus for each section. Start the subjective section with the patient’s chief complaint and include relevant medical history when it directly affects clinical decision-making, such as prior surgeries or comorbidities.
For the objective section, use specific numbers for each data point, goniometric measurements of ROM with normal reference values, and the standard 0-5 manual muscle testing scale for strength.
The assessment section is where many therapy SOAP notes fall short. Restating findings is not an assessment. A complete assessment includes the clinical impression, a statement of progress toward functional goals, and the justification for continued skilled care.
It should address the patient’s condition directly, explaining what the findings mean for function and why the current level of care remains appropriate. For the plan section, state the next session date or frequency, list home exercises with specific parameters, and note any referrals or changes to the treatment plan.
Physical Therapy SOAP Note Examples
Reviewing a soap note example from physiotherapy alongside your own documentation is a practical way to identify gaps in clinical detail or reasoning. The examples below cover the most common note types in outpatient PT and illustrate how content varies across conditions, stages of care, and patient populations.
Physical Therapy Initial Evaluation SOAP Note Example
S: Patient is a 42-year-old male referred for low back pain following a workplace lifting injury three weeks ago. Reports pain at 7/10 at rest, 9/10 with bending. Unable to sit for more than 20 minutes. No radiating symptoms. Medical history includes no prior lumbar injury or surgery. The goal is to return to full work duties.
O: Lumbar flexion AROM: 30 degrees (normal: 60 degrees). Lumbar extension AROM: 10 degrees (normal: 25 degrees). Straight leg raise negative bilaterally. Palpation reveals tenderness at L4-L5 paraspinal musculature. No neurological deficits noted—Oswestry Disability Index score: 42% (moderate disability).
A: Patient presents with acute lumbar strain with significant ROM limitations and pain-limited functional tolerance, consistent with the mechanism of injury. Goals: reduce pain to 3/10, restore functional ROM, and return to full work duties within six weeks.
P: Three sessions per week for four weeks. The treatment plan includes manual therapy, core stabilization exercises, and patient education on body mechanics. Home exercise program provided. Reassess the full ROM and ODI score in two weeks.

Physical Therapy Daily SOAP Note Example: Acute Low Back Pain
S: Patient reports pain at 5/10 today, down from 7/10 at last session. Able to sit for 30 minutes before pain onset. Completed home exercises four out of seven days.
O: Lumbar flexion AROM: 42 degrees (improved from 30 degrees at initial eval). Extension AROM: 18 degrees (improved from 10 degrees). Soft tissue mobilization at L4-L5 bilaterally for 10 minutes. Therapeutic exercise: pelvic tilts 3×15, bird-dog 3×10 each side, bridging 3×15.
A: Patient demonstrates measurable improvement in ROM and pain levels after two sessions. Progressing toward functional goals at the expected rate. Continued skilled PT indicated to address remaining deficits and reinforce body mechanics for work tasks.
P: Continue current plan. Progress core exercise difficulty at next session. Reassess the full ROM and ODI score at session six.

Physical Therapy Daily SOAP Note Example: Shoulder Impingement
S: Patient reports pain at 4/10 with overhead reaching, improved from 7/10 at initial evaluation. Difficulty with dressing and reaching overhead cabinets persists.
O: Shoulder flexion AROM: 145 degrees (improved from 120 degrees; normal: 180 degrees). Abduction AROM: 130 degrees (improved from 105 degrees; normal: 180 degrees). Hawkins-Kennedy test: positive. Rotator cuff strength: 4/5 in all planes. Manual therapy to the posterior capsule was performed. Strengthening exercises: side-lying external rotation, 3×15 at 2 lbs; scapular retraction, 3×15.
A: Patient shows continued ROM gains and improved functional tolerance since the initial evaluation. Impingement symptoms persist with overhead loading. Skilled PT indicated to address remaining rotator cuff deficits and reach the functional goal of pain-free overhead activity.
P: Progress to standing cable external rotation at next session. Continue posterior capsule stretching as part of the home program.

Pediatric Physical Therapy SOAP Note Example
S: Parent reports child (age 7) has difficulty keeping up with peers during recess. Child reports right knee pain at 3/10 during running—no recent injury. Symptoms present for approximately six weeks.
O: Gait assessment: reduced right hip extension and increased contralateral trunk lean. Single-leg squat: right knee valgus collapse noted. Hip abductor strength: 3/5 right, 4/5 left. Timed Up and test: 14 seconds (age-expected range: 8 to 10 seconds). Therapeutic exercise: clamshells 3×12, lateral band walks 2×10, single-leg balance 3×20 seconds.
A: Child presents with right knee pain consistent with hip abductor weakness and dynamic valgus during weight-bearing activity. No signs of acute pathology. Goals: improve hip strength to 4+/5, eliminate valgus collapse with single-leg tasks, and return to full recess participation.
P: Two sessions per week for four weeks. Progress strengthening exercises and introduce running mechanics training at the next session—a written home program will be provided to the parent.

SOAP Note vs. Progress Note vs. Evaluation Note
These three documents each serve a different function in a PT record.
| Document | Purpose | When to Use |
|---|---|---|
| Initial Evaluation Note | Full examination, diagnosis, and plan of care | First visit only |
| Daily SOAP Note | Record of each treatment session | Every session after evaluation |
| Progress Note | Summary of patient progress and updated goals | Every 10 visits or payer required |
The progress note is a periodic summary that justifies continued care to insurers and formally updates the plan of care, not a session-by-session record. Conflating the two is a common documentation error that can create billing problems.
Common SOAP Note Mistakes and How to Fix Them
- Being too vague in the objective section. Entries like “patient performed exercises” or “ROM improved” provide no measurable data. Fix: use specific numbers, exercise parameters, and named tests with normal reference values in every note.
- Skipping clinical reasoning in the assessment. “Patient tolerated treatment well” describes the session without interpreting it. Fix: state the patient’s current clinical status, progress toward functional goals, and the reason skilled PT remains necessary.
- Copy-pasting notes between sessions. Copied notes create a false record and a compliance risk. Fix: write each note from the actual session findings, even when changes are small.
- Overusing abbreviations. Heavy use creates problems for outside reviewers. Fix: spell out any term not universally recognized in PT practice.
SOAP Notes, Billing, and Medical Necessity
Medical necessity means the treatment provided was clinically required at that specific point in the patient’s care. A soap note template can help organize the format, but the clinical content still needs to be specific to that patient on that day. Every note should answer the question: why did this patient need a licensed PT today rather than a home exercise program alone?
Skilled care means treatment that requires the training, clinical judgment, and decision-making of a licensed physical therapist. The note must show the reasoning behind each clinical choice, the patient’s response, and how the session connected to the patient’s functional goals.
Including standardized outcome measure scores at baseline and at reassessment, such as the Oswestry Disability Index or the Lower Extremity Functional Scale, provides insurers and auditors with quantifiable evidence that the patient’s treatment was producing measurable results.
A well-written physical therapy notes record is the clearest way to demonstrate that skilled care was delivered, that patient outcomes were tracked, and that the patient’s treatment was individualized to their condition from the first session to the last.
For physical therapists working in outpatient settings across New York City, this level of documentation is both a professional standard and a billing requirement. If you are looking for a ready-to-use format, a physical therapy SOAP note template can serve as a starting point, but every field still needs to reflect the specific clinical picture of that session.

