
Keith Chan is a New York State-licensed physical therapist at ITNYCPT. He works with patients across New York City, managing FAI through individualized rehab programs.
This guide explains the condition, how physical therapy treats it, and what a structured exercise program looks like.
Key Takeaways
- Femoroacetabular impingement (FAI) is diagnosed through a combination of imaging, clinical tests, and reported symptoms – imaging findings alone are not sufficient, since cam morphology appears in roughly 22% of people with no pain at all.
- Physical therapy is the appropriate first-line treatment for most people with FAI. Three randomized controlled trials found no significant difference between surgery and PT at two years, and fewer than 20% of surgical patients return to their prior athletic performance level.
- Effective FAI rehab targets all major hip muscle groups – extensors, abductors, adductors, flexors, and hamstrings – progressing over at least 3 months, with 2-3 sessions per week, starting with isometric holds and advancing to loaded repetitions.
- Certain movements consistently provoke FAI symptoms by loading the hip at end range, including deep squats below parallel, full-depth leg press, and high-knee drills. The goal is to modify these movements, not eliminate them permanently.
- Most patients see meaningful improvement within 3 to 6 months of structured rehab, though recovery timelines vary based on symptom severity, training history, consistency, and overall health.
What Is Femoroacetabular Impingement?
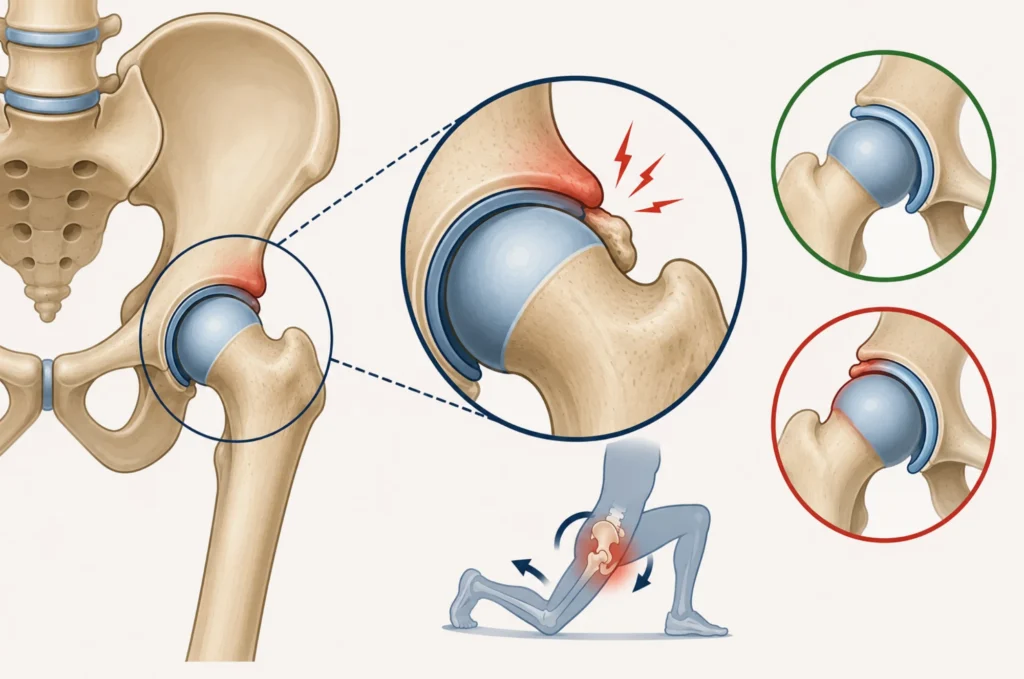
Femoroacetabular impingement (FAI) is a condition where the femoral head rubs against the acetabulum during movement – the ball-and-socket of the hip joint.
That contact creates friction, which, over time, irritates nearby structures, including the labrum and cartilage, causing hip joint pain, stiffness, and reduced range of motion.
Symptoms typically appear at the extremes of hip flexion and internal rotation, during activities such as deep squats, prolonged sitting, stair climbing, and sports.
Cam, Pincer, and Mixed Morphology: What the Types Mean
Cam morphology refers to an irregular shape at the femoral head, pincer morphology refers to excess coverage by the acetabulum, and mixed morphology combines both. Each type affects the hip joint differently, but all three produce similar symptoms with varying loads and movements.
Diagnosis requires imaging, clinical signs, and reported symptoms together. A 2016 systematic review by Vasco V. Mascarenhas found cam morphology in 22% of asymptomatic individuals, confirming that imaging findings alone are insufficient to establish a diagnosis.
Symptoms, Clinical Signs, and How FAI Is Diagnosed
The FADIR test – hip flexion, adduction, and internal rotation – is the most widely used clinical provocation test for FAI. FABER testing – abduction and external rotation – evaluates symptoms and side-to-side differences in range of motion.
A physical therapist uses the full clinical picture alongside X-ray or MRI findings to guide treatment, not imaging alone.
Can Physical Therapy Fix Hip Impingement?
Yes. Physical therapy cannot change the bone shape that causes FAI, but it can reduce pain and restore function in most cases without surgery.
Three randomized controlled trials – by Damian R. Griffin, Nancy S. Mansell, and Antony J. R. Palmer – compared arthroscopic hip surgery with physical therapy. A 2020 meta-analysis by Joanne L. Kemp pooled the data and found that surgery produced a small benefit at 8-12 months, but no significant difference at two years.
Research by Lasse Ishøi and Kristian Thorborg found that only around 50-60% of surgical patients report acceptable outcomes, and fewer than 20% return to their prior level of athletic performance, making physical therapy the appropriate first-line treatment for most people.
Femoroacetabular Impingement Physical Therapy Protocol
A PT evaluation for FAI begins with a patient history, movement screen, range-of-motion testing, and strength assessment, followed by an individualized plan of care.
Sessions typically include therapeutic exercise, manual therapy, and guidance on activity modification. In some cases, the Graston Technique is used to address soft tissue restrictions around the hip.
The first step in any protocol is to identify provocative activities and find tolerable alternatives to keep the patient active while reducing irritation. Common substitutions include:
- Box squats or heel-elevated squats instead of full-depth back squats
- Trap bar or Romanian deadlifts instead of conventional pulls
- Split squats when bilateral loading is too provocative
- Swimming or cycling when impact-based training needs to be reduced
The Best Exercises for Femoroacetabular Impingement
Hip muscle weakness is a central and consistent finding in FAI. A 2016 systematic review by Matthew D. Freke confirmed measurable deficits in hip strength and single-leg balance among symptomatic patients.
Research by Lasse Ishøi further found that higher muscle strength was positively associated with better sports function after hip surgery – reinforcing that strengthening is the core of conservative rehab.
Exercises for FAI impingement need to address all major muscle groups around the hip and be progressed over at least 3 months, with 2-3 sessions per week.
One rule applies to all of them: stay at a pain level of 2 or less out of 10. Begin with isometric holds at 3 sets of 60 seconds, then advance to 3 sets of 8-15 controlled repetitions under load.
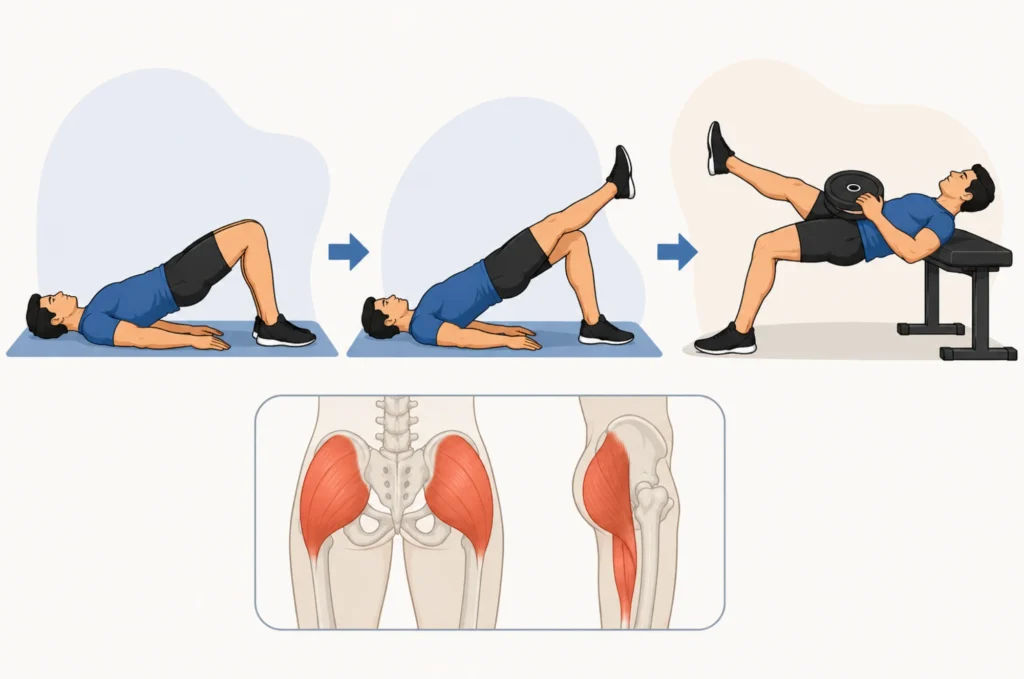
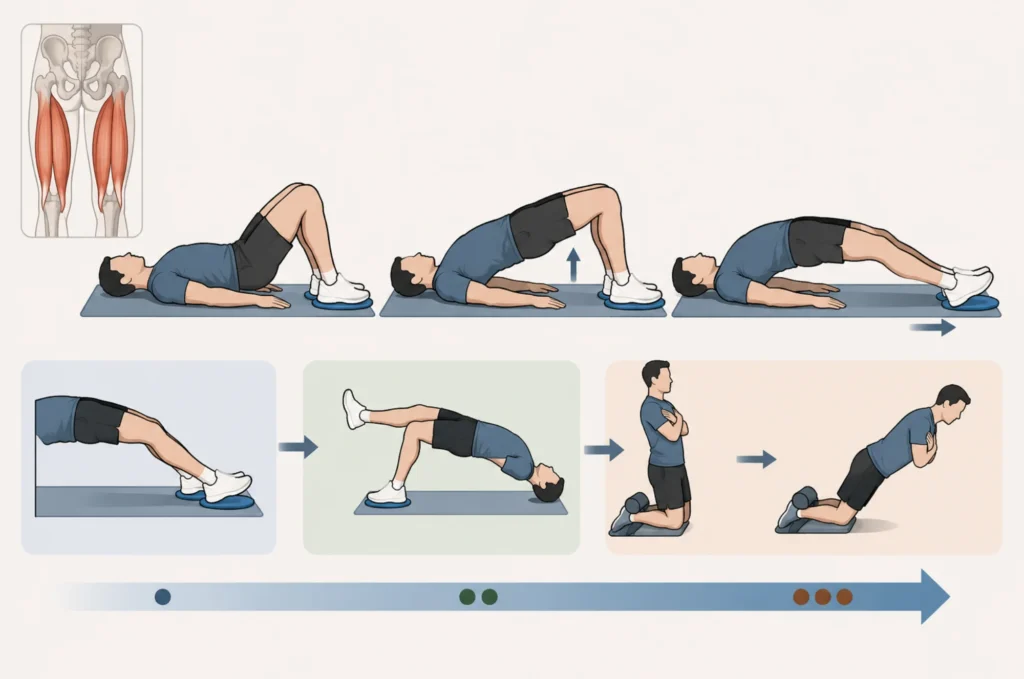
Hip Extensors: Bridges and Single-Leg Hip Thrusts
Hip extensor weakness increases the stress the hip joint absorbs on every step, making this the most important muscle group to address early in FAI rehab.
From your start position – lying on your back with feet flat and knees bent – drive the hips toward the ceiling until your body forms a straight line from shoulders to knees.
Progress from a double-leg bridge isometric to single-leg variations, then to a weighted single-leg hip thrust with the upper back elevated on a bench. Training hip extension keeps the load away from the provocative flexion range while building the strength needed for daily movement and sport.
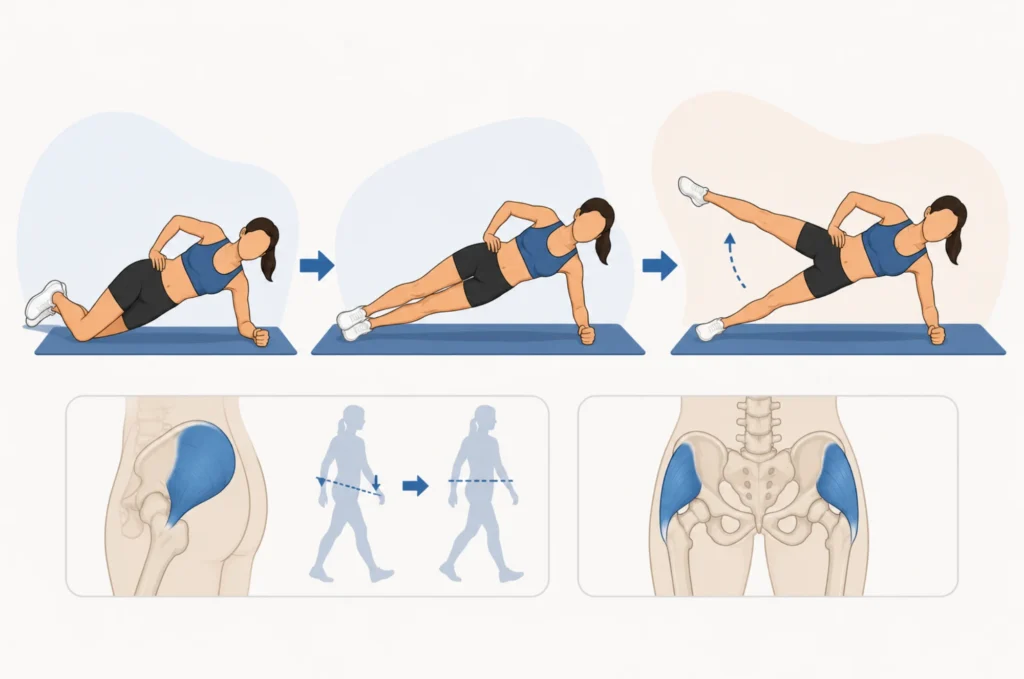
Hip Abductors: Side Planks and Hip Abduction
The gluteus medius controls pelvic stability during single-leg loading. Weakness here causes a pelvic drop during walking and running, increasing compressive forces at the hip joint and worsening FAI symptoms over time.
Start with a short side plank from the knees – forearm on the floor, hips lifted, body in a straight line from knees to shoulders. Progress to a full side plank from the feet, then add controlled hip abduction by slowly lifting the top leg.
Improving hip health through abductor training directly reduces abnormal joint loading – weakness in this area is also associated with conditions like greater trochanteric pain syndrome, which affects the outer hip.
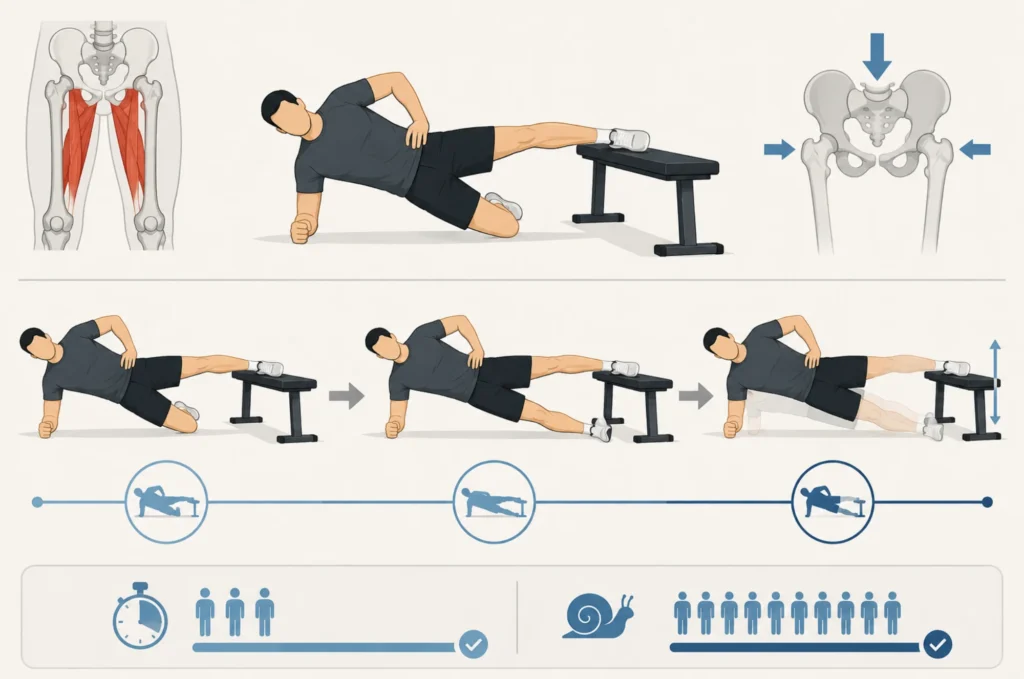
Hip Adductors: Copenhagen Plank Progressions
The adductors contribute directly to hip joint compression and stability, yet they are routinely skipped in hip rehab programs. Set up in a side-lying position with the top foot resting on a bench, body in a straight line, and lift the hips to hold a short Copenhagen plank isometric.
Progress to a long Copenhagen plank by straightening the bottom leg, which substantially increases adductor demand. Once 3 sets of 60-second holds are manageable, introduce slow repetitions targeting 3 sets of 8-12.
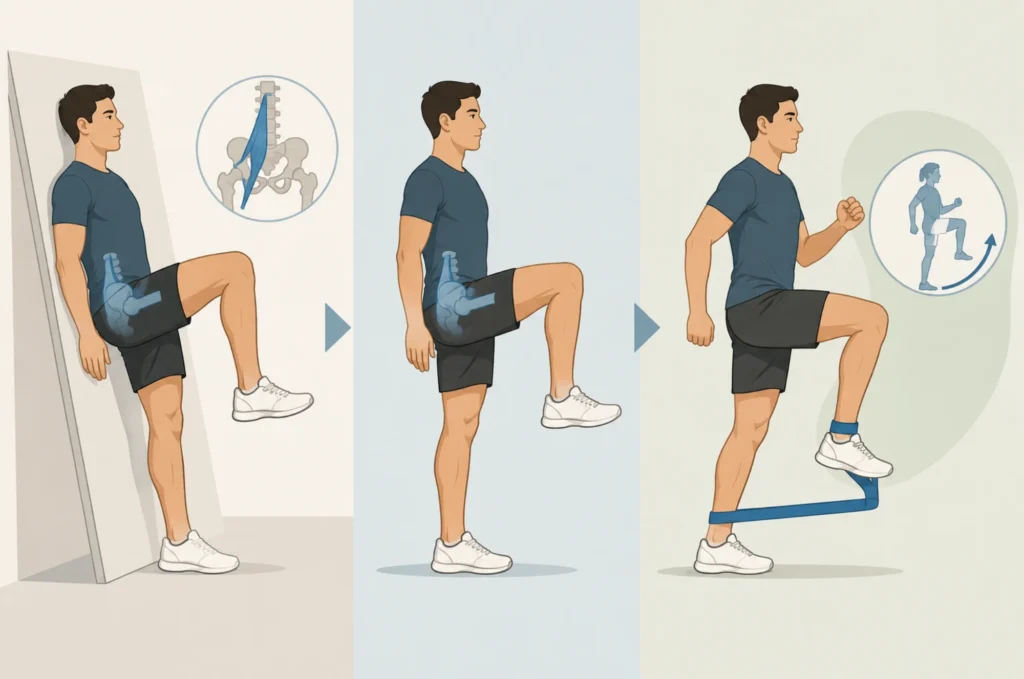
Hip Flexors: Standing and Incline Isometrics
Weakness in the hip flexors – particularly the iliopsoas – reduces control of the femoral head within the socket, worsening the impingement pattern during any activity requiring hip flexion.
Start with an incline hip flexion isometric: back against a wall, one thigh lifted to 90 degrees of hip flexion, held without hand support.
Progress to a standing isometric, then banded marching with a resistance loop around the ankles, targeting 3 sets of 10-15 deliberate repetitions. This approach systematically reintroduces hip flexion range of motion in a load-tolerant way while supporting long-term hip health.
Hamstrings: Sliders and Nordic Curls
The hamstrings cross both the hip and the knee, and in FAI rehab, they are trained in hip extension to avoid loading the provocative flexion range. Bridge up from your start position on the floor with feet on sliders or towels, then slowly slide both feet out while maintaining hip height – this is the double-leg eccentric slider.
The eccentric slide places the hamstrings under high load in a hip-extended position. Progress to single-leg sliders, then Nordic hamstring curls, targeting 3 sets of 4-8 repetitions, given the high demand involved.
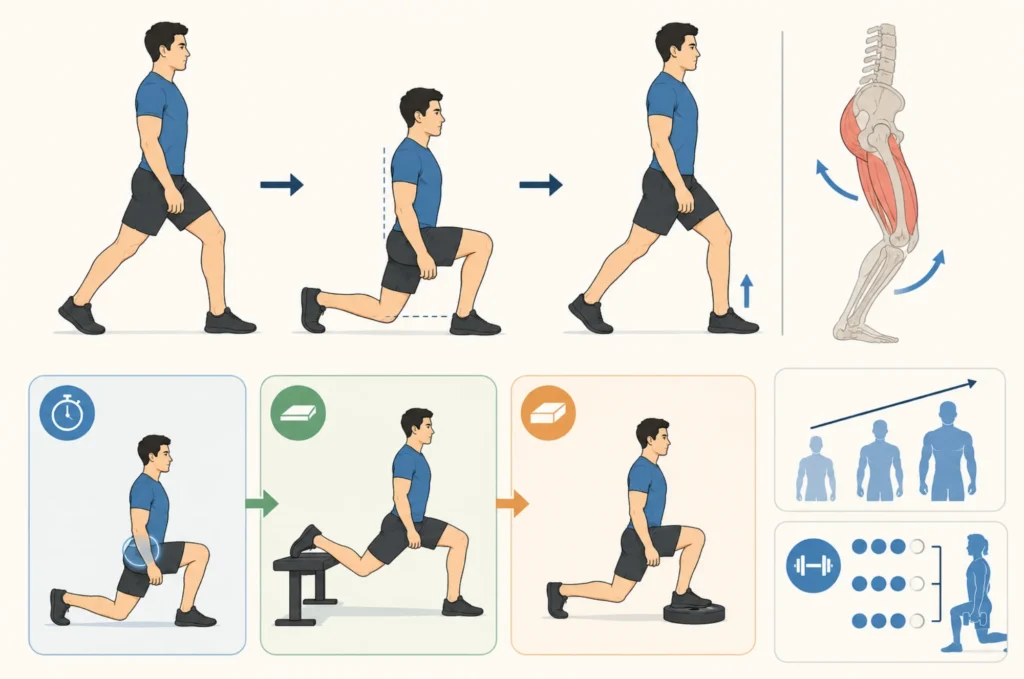
Split Squats: Training the Hip and Knee Together
The split squat trains hip and knee extension together while allowing precise control over hip flexion depth – making it one of the most useful exercises for FAI impingement when bilateral squatting is too provocative. Stand in a staggered stance, lower until the rear knee hovers just above the floor with the torso upright, then drive back up through the front heel.
Begin with bodyweight isometric holds at the bottom, progress to a rear-foot-elevated variation, then gradually add a front-foot deficit to increase hip flexion range under load. Target 3 sets of 6-12 repetitions with added weight as strength develops.
Plyometric and Sport-Specific Progressions
Strength training alone does not replicate the demands of running, cutting, jumping, or pivoting. For patients returning to sport, plyometric work needs to be built into the plan of care well before clearance – not added at the last minute.
Begin with low-level hops and bounds, advance to single-leg landing mechanics, then progress through cutting, tempo running, and full-speed sport-specific drills. Skipping this phase is one of the most common reasons patients stall before returning to full activity.

Hip Impingement Exercises to Avoid
Movements That Load the Hip at End Range
Certain movements drive the femoral head into contact with the acetabulum at end range and consistently provoke FAI symptoms. The most common ones to reduce or temporarily remove include:
- Deep squats below parallel, particularly with a narrow stance
- High-knee running drills with excessive hip flexion
- Leg press at full depth with knees driven toward the chest
- Wide-stance sumo deadlifts combine hip flexion with external rotation
- Seated hip flexion exercises loading the hip at or past 90 degrees
These are not permanent exclusions. The goal of FAI rehab is to build enough capacity that many of these movements become tolerable again over time.
How to Modify Instead of Stopping Altogether
Complete avoidance is rarely the answer. A physical therapist identifies the specific range of motion that provokes symptoms and adjusts the movement accordingly – shortening squat depth, changing stance width, reducing load, or switching to a machine-based alternative.
This maintains training volume while protecting the hip joint during the early and middle phases of rehab.
Hip Impingement Stretches and Mobility Work
Stretches for FAI: Hip Flexor, Piriformis, and Groin
Femoroacetabular impingement stretches target the muscles that tighten as a result of guarding, and improving hip mobility through targeted stretching is one way to maintain range of motion between strengthening sessions.
Stretches for FAI support the strengthening work by improving access to a range rangea of motion before and after sessions – they are not the primary driver of recovery. The three most commonly prescribed are:
- Hip flexor stretch: half-kneeling, rear knee down, hips pushed gently forward, held 20-30 seconds
- Piriformis stretch: lying on your back, ankle crossed over the opposite bent knee, thigh pulled toward the chest
- Groin stretch: seated butterfly, soles of the feet together, knees dropping toward the floor
Perform each for 20-30 seconds, 3 times per side, and avoid any position that reproduces hip joint pain.
What Stretching Can and Cannot Do for FAI
Stretching and banded mobilizations can reduce stiffness, improve comfort during daily activity, and help patients access a slightly greater range of motion for training. What they cannot do is correct underlying muscle weakness or structural changes driving FAI symptoms.
Passive flexibility work earns its place in an FAI program when it supports the strengthening work, not when it substitutes for it.
Will You Be Able to Exercise Normally Again?
Most patients following a structured FAI rehab program see meaningful improvement within 3 to 6 months. Recovery timelines vary based on symptom severity, condition duration, training history, home exercise consistency, sleep, and overall health.
Return to sport is a process – most athletes need a structured progression through running, plyometrics, and sport-specific drills before returning to full competition.
Research by Lasse Ishøi found that 57% of individuals returned to their pre-injury sport, but only 17% returned to their prior performance level nearly three years after surgery. For those who do eventually require an operation, physical therapy for hip replacement follows its own structured recovery protocol.
Conservative rehab, applied thoroughly and progressively, gives most patients a realistic path back to full activity without those trade-offs.

